With stroke becoming the main cause of global morbidity and mortality. The urgent demand for reliable biomarkers to enhance prognostic accuracy and guide individualized clinical decision-making has never been more pronounced. This unmet need is amplified by the disease’s heterogeneous etiologies and variable clinical trajectories, which often hinder timely risk stratification and targeted intervention for stroke patients. A growing body of research has delved into diverse categories of candidate biomarkers, encompassing inflammatory mediators, metabolic indicators, and blood cellular parameters and evaluated their potential in predicting short-term and long-term stroke outcomes such as functional independence, recurrence risk, and mortality. Through a narrative review of current literature, we have summarized key biomarkers such as C-reactive protein, interleukins, blood cells, lipid profiles, oxidative stress markers, microparticles and cell-free DNA, clarifying their associations with stroke pathophysiology and clinical endpoints. Simultaneously, we highlighted critical gaps and inconsistencies in existing studies, such as limited validation in multiethnic and underrepresented patient cohorts. Furthermore, we have discussed the practical clinical applications and inherent challenges of translating these biomarkers into real-world settings. Finally, we have proposed future research directions, emphasizing the development of standardized protocols, validation in large-scale prospective cohorts, and exploration of multiple biomarkers to address unmet clinical needs in stroke management.
| Published in | International Journal of Neurosurgery (Volume 9, Issue 2) |
| DOI | 10.11648/j.ijn.20250902.12 |
| Page(s) | 49-59 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Biomarkers, Prognosis, Clinical Decision-making, Peripheral Blood Markers, Stroke
Peripheral blood markers | Good prognosis |
|---|---|
C-Reactive Protein (CRP) | Negative |
Interleukin-6 (IL-6) | Negative |
Interleukin-10 (IL-10) | Positive |
Neutrophil-to-Lymphocyte Ratio (NLR) | Negative |
Low-density lipoprotein cholesterol (LDL-C) | Negative |
Residual cholesterol (RC) | Negative |
Reactive oxygen species (ROS) | Negative |
Microparticles | Negative |
Cell-free DNA | Negative |
Fibrinogen | Positive |
ATP | Adenosine Triphosphate |
BBB | Blood-brain Barrier |
CRP | C-Reactive Protein |
CT | Computed Tomography |
IL-6 | Interleukin-6 |
IL-10 | Interleukin-10 |
LDL-C | Low-density Lipoprotein Cholesterol |
MRI | Magnetic Resonance Imaging |
mRS | modified Rankin Scale |
NHHR | High-density LIPoprotein Cholesterol Ratio |
NIHSS | National Institutes of Health Stroke Scale |
NLR | Neutrophil-to-Lymphocyte Ratio |
NMDA | N-Methyl-D-Aspartic Acid |
RC | Residual Cholesterol |
ROS | Reactive Oxygen Species |
sICH | Symptomatic Intracranial Hemorrhage |
| [1] | Feigin VL, Norrving B, Mensah GA. Global Burden of Stroke. Circ Res. 2017, 120(3), 439-448. |
| [2] | Nehme A, Li L. The rising incidence of stroke in the young: Epidemiology, causes and global impact. Int J Stroke. Published online July 18, 2025. |
| [3] | Montaño A, Hanley DF, Hemphill JC 3rd. Hemorrhagic stroke. Handb Clin Neurol. 2021, 176, 229-248. |
| [4] | Campbell BCV, De Silva DA, Macleod MR, Coutts SB, Schwamm LH, Davis SM, et al. Ischaemic stroke. Nat Rev Dis Primers. 2019, 5(1), 70. |
| [5] | Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2021, 52(7), e364-e467. |
| [6] | Whiteley W, Chong WL, Sengupta A, Sandercock P. Blood markers for the prognosis of ischemic stroke: a systematic review. Stroke. 2009, 40(5), e380-389. |
| [7] | Branco JP, Costa JS, Sargento-Freitas J, Oliveira S, Mendes B, Laíns J, et al. Neuroimaging and Blood Biomarkers in Functional Prognosis after Stroke. Acta Med Port. 2016, 29(11), 749-754. |
| [8] | Tirandi A, Sgura C, Carbone F, Montecucco F, Liberale L. Inflammatory biomarkers of ischemic stroke. Intern Emerg Med. 2023, 18(3), 723-732. |
| [9] | Alsbrook DL, Di Napoli M, Bhatia K, Biller J, Andalib S, Hinduja A, et al. Neuroinflammation in Acute Ischemic and Hemorrhagic Stroke. Curr Neurol Neurosci Rep. 2023, 23(8), 407-431. |
| [10] | Ma X, Lan F, Zhang Y. Associations between C-reactive protein and white blood cell count, occurrence of delayed cerebral ischemia and poor outcome following aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. Acta Neurol Belg. 2021, 121(5), 1311-1324. |
| [11] | Guo P, Zou W. Neutrophil-to-lymphocyte ratio, white blood cell, and C-reactive protein predicts poor outcome and increased mortality in intracerebral hemorrhage patients: a meta-analysis. Front Neurol. 2024, 14, 1288377. |
| [12] | Wang L, Yang L, Liu H, Pu J, Li Y, Tang L, et al. C-Reactive Protein Levels and Cognitive Decline following Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Brain Sci. 2023, 13(7), 1082. |
| [13] | Denegri A, Boriani G. High Sensitivity C-reactive Protein (hsCRP) and its Implications in Cardiovascular Outcomes. Curr Pharm Des. 2021, 27(2), 263-275. |
| [14] | Fu Y, Wu Y, Liu E. C-reactive protein and cardiovascular disease: From animal studies to the clinic (Review). Exp Ther Med. 2020, 20(2), 1211-1219. |
| [15] | Yang T, Xie W, Hu F, Cai B. Causal relationship between C-reactive protein and ischemic stroke caused by atherosclerosis: A Mendelian randomization study. J Stroke Cerebrovasc Dis. 2024, 33(9), 107873. |
| [16] | Gaastra B, Barron P, Newitt L, Chhugani S, Turner C, Kirkpatrick P, et al.CRP (C-Reactive Protein) in Outcome Prediction After Subarachnoid Hemorrhage and the Role of Machine Learning. Stroke. 2021, 52(10), 3276-3285. |
| [17] | Tang Y, Fung E, Xu A, Lan HY. C-reactive protein and ageing. Clin Exp Pharmacol Physiol. 2017, 44 (Suppl 1), 9-14. |
| [18] | Qiu R, Gao Y, Hou D, Wang Y, Yu C, Wang W, et al. Association between hs-CRP Levels and the Outcomes of Patients with Small-Artery Occlusion. Front Aging Neurosci. 2016, 8, 191. |
| [19] | Zhu H, Hu S, Li Y, Sun Y, Xiong X, Hu X, et al. Interleukins and Ischemic Stroke. Front Immunol. 2022, 13, 828447. |
| [20] | Peng L, Li X, Li H, Zhong Y, Lian J, Gao H, et al. Relationship between Peripheral Blood Inflammatory Factors and Prognosis of Subarachnoid Hemorrhage: A Meta-Analysis. Eur Neurol. 2023, 86(3), 193-206. |
| [21] | Simon M, Grote A. Interleukin 6 and Aneurysmal Subarachnoid Hemorrhage. A Narrative Review. Int J Mol Sci. 2021, 22(8), 4133. |
| [22] | Tschoe C, Bushnell CD, Duncan PW, Alexander-Miller MA, Wolfe SQ. Neuroinflammation after Intracerebral Hemorrhage and Potential Therapeutic Targets. J Stroke. 2020, 22(1), 29-46. |
| [23] | Huang X, Zhang M, Wang J, Hu F. Association between interleukin-6 levels and stroke: a systematic review and meta-analysis. J Int Med Res. 2024, 52(9), 3000605241274626. |
| [24] | Wu W, Luo Z, Shen D, Lan T, Xiao Z, Liu M, et al. IL-10 protects against OPC ferroptosis by regulating lipid reactive oxygen species levels post stroke. Redox Biol. 2024, 69, 102982. |
| [25] | Sarejloo S, Kheradjoo H, Haghi SE, Hosseini S, Gargari MK, Azarhomayoun A, et al. Neutrophil-to-Lymphocyte Ratio and Early Neurological Deterioration in Stroke Patients: A Systematic Review and Meta-Analysis. Biomed Res Int. 2022, 2022, 8656864. |
| [26] | Luo Y, Zhao J. The dynamic changes of peripheral blood cell counts predict the clinical outcomes of aneurysmal subarachnoid hemorrhage. Heliyon. 2024, 10(8), e29763. |
| [27] | Luo Y, Xia LX, Li ZL, Pi DF, Tan XP, Tu Q. Early neutrophil-to-lymphocyte ratio is a prognostic marker in acute minor stroke or transient ischemic attack. Acta Neurol Belg. 2021, 121(6), 1415-1421. |
| [28] | Lattanzi S, Brigo F, Trinka E, Cagnetti C, Di Napoli M, Silvestrini M. Neutrophil-to-Lymphocyte Ratio in Acute Cerebral Hemorrhage: a System Review. Transl Stroke Res. 2019, 10(2), 137-145. |
| [29] | Shi M, Yang C, Tang QW, Xiao LF, Chen ZH, Zhao WY. The Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Patients With Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis of Observational Studies. Front Neurol. 2021, 12, 745560. |
| [30] | Alloubani A, Nimer R, Samara R. Relationship between Hyperlipidemia, Cardiovascular Disease and Stroke: A Systematic Review. Curr Cardiol Rev. 2021, 17(6), e051121189015. |
| [31] | Ma HX, Chen HQ, Wang PC. Association between Non-high-density Lipoprotein Cholesterol to High-density Lipoprotein Cholesterol Ratio (NHHR) and Stroke among Adults in the USA: A Cross-Sectional NHANES Study. Biomed Environ Sci. 2025, 38(1), 37-46. |
| [32] | Yang B, Ma X, Yang L, Bian G, Qiao B, Lu H, et al.Trends and Prospects of Low-Density Lipoprotein Cholesterol in Stroke: A Bibliometric Analysis. Cureus. 2024, 16(9), e69492. |
| [33] | Aznaouridis K, Masoura C, Vlachopoulos C, Tousoulis D. Statins in Stroke. Curr Med Chem. 2019, 26(33), 6174-6185. |
| [34] | Sanz-Cuesta BE, Saver JL. Lipid-Lowering Therapy and Hemorrhagic Stroke Risk: Comparative Meta-Analysis of Statins and PCSK9 Inhibitors. Stroke. 2021, 52(10), 3142-3150. |
| [35] | Kamal FZ, Lefter R, Jaber H, Balmus IM, Ciobica A, Iordache AC. The Role of Potential Oxidative Biomarkers in the Prognosis of Acute Ischemic Stroke and the Exploration of Antioxidants as Possible Preventive and Treatment Options. Int J Mol Sci. 2023, 24(7), 6389. |
| [36] | Briyal S, Ranjan AK, Gulati A. Oxidative stress: A target to treat Alzheimer's disease and stroke. Neurochem Int. 2023, 165, 105509. |
| [37] | Yang Y, Li Z, Fan X, Jiang C, Wang J, Rastegar-Kashkooli Y, et al. Nanozymes: Potential Therapies for Reactive Oxygen Species Overproduction and Inflammation in Ischemic Stroke and Traumatic Brain Injury. ACS Nano. 2024, 18(26), 16450-16467. |
| [38] | Kalogeris T, Baines CP, Krenz M, Korthuis RJ. Ischemia/Reperfusion. Compr Physiol. 2016, 7(1), 113-170. |
| [39] | Li P, Stetler RA, Leak RK, Shi Y, Li Y, Yu W, et al. Oxidative stress and DNA damage after cerebral ischemia: Potential therapeutic targets to repair the genome and improve stroke recovery. Neuropharmacology. 2018, 134(Pt B), 208-217. |
| [40] | Tao T, Liu M, Chen M, Luo Y, Wang C, Xu T, et al. Natural medicine in neuroprotection for ischemic stroke: Challenges and prospective. Pharmacol Ther. 2020, 216, 107695. |
| [41] | Maggio E, Bocchini VP, Carnevale R, Pignatelli P, Violi F, Loffredo L. Vitamin E supplementation (alone or with other antioxidants) and stroke: a meta-analysis. Nutr Rev. 2024, 82(8), 1069-1078. |
| [42] | Bavarsad Shahripour R, Harrigan MR, Alexandrov AV. N-acetylcysteine (NAC) in neurological disorders: mechanisms of action and therapeutic opportunities. Brain Behav. 2014, 4(2), 108-122. |
| [43] | El-Gamal H, Parray AS, Mir FA, Shuaib A, Agouni A. Circulating microparticles as biomarkers of stroke: A focus on the value of endothelial- and platelet-derived microparticles. J Cell Physiol. 2019, 234(10), 16739-16754. |
| [44] | Hayon Y, Shai E, Varon D, Leker RR. The role of platelets and their microparticles in rehabilitation of ischemic brain tissue. CNS Neurol Disord Drug Targets. 2012, 11(7), 921-925. |
| [45] | Roth S, Wernsdorf SR, Liesz A. The role of circulating cell-free DNA as an inflammatory mediator after stroke. Semin Immunopathol. 2023, 45(3), 411-425. |
| [46] | Glebova KV, Veiko NN, Nikonov AA, Porokhovnik LN, Kostuyk SV. Cell-free DNA as a biomarker in stroke: Current status, problems and perspectives. Crit Rev Clin Lab Sci. 2018, 55(1), 55-70. |
| [47] | Youyou Z, Ruirui J, Hui W, Zhaoyang L. Association between lipoprotein(a) and ischemic stroke: Fibrinogen as a mediator. J Neurol Sci. 2023, 452, 120738. |
| [48] | Li X, Du H, Song Z, Meiqi, Zhang G, Yuan S, et al. Association between fibrinogen levels and stroke-associated pneumonia in acute ischemic stroke patients. BMC Neurol. 2024, 24(1), 256. |
APA Style
Zeng, Z., Wang, L., Zhu, S., Luo, Y. (2025). A Narrative Review of Peripheral Blood Markers for Stroke Prognosis. International Journal of Neurosurgery, 9(2), 49-59. https://doi.org/10.11648/j.ijn.20250902.12
ACS Style
Zeng, Z.; Wang, L.; Zhu, S.; Luo, Y. A Narrative Review of Peripheral Blood Markers for Stroke Prognosis. Int. J. Neurosurg. 2025, 9(2), 49-59. doi: 10.11648/j.ijn.20250902.12
@article{10.11648/j.ijn.20250902.12,
author = {Ziquan Zeng and Lu Wang and Shaoliang Zhu and Yi Luo},
title = {A Narrative Review of Peripheral Blood Markers for Stroke Prognosis},
journal = {International Journal of Neurosurgery},
volume = {9},
number = {2},
pages = {49-59},
doi = {10.11648/j.ijn.20250902.12},
url = {https://doi.org/10.11648/j.ijn.20250902.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijn.20250902.12},
abstract = {With stroke becoming the main cause of global morbidity and mortality. The urgent demand for reliable biomarkers to enhance prognostic accuracy and guide individualized clinical decision-making has never been more pronounced. This unmet need is amplified by the disease’s heterogeneous etiologies and variable clinical trajectories, which often hinder timely risk stratification and targeted intervention for stroke patients. A growing body of research has delved into diverse categories of candidate biomarkers, encompassing inflammatory mediators, metabolic indicators, and blood cellular parameters and evaluated their potential in predicting short-term and long-term stroke outcomes such as functional independence, recurrence risk, and mortality. Through a narrative review of current literature, we have summarized key biomarkers such as C-reactive protein, interleukins, blood cells, lipid profiles, oxidative stress markers, microparticles and cell-free DNA, clarifying their associations with stroke pathophysiology and clinical endpoints. Simultaneously, we highlighted critical gaps and inconsistencies in existing studies, such as limited validation in multiethnic and underrepresented patient cohorts. Furthermore, we have discussed the practical clinical applications and inherent challenges of translating these biomarkers into real-world settings. Finally, we have proposed future research directions, emphasizing the development of standardized protocols, validation in large-scale prospective cohorts, and exploration of multiple biomarkers to address unmet clinical needs in stroke management.},
year = {2025}
}
TY - JOUR T1 - A Narrative Review of Peripheral Blood Markers for Stroke Prognosis AU - Ziquan Zeng AU - Lu Wang AU - Shaoliang Zhu AU - Yi Luo Y1 - 2025/12/31 PY - 2025 N1 - https://doi.org/10.11648/j.ijn.20250902.12 DO - 10.11648/j.ijn.20250902.12 T2 - International Journal of Neurosurgery JF - International Journal of Neurosurgery JO - International Journal of Neurosurgery SP - 49 EP - 59 PB - Science Publishing Group SN - 2640-1959 UR - https://doi.org/10.11648/j.ijn.20250902.12 AB - With stroke becoming the main cause of global morbidity and mortality. The urgent demand for reliable biomarkers to enhance prognostic accuracy and guide individualized clinical decision-making has never been more pronounced. This unmet need is amplified by the disease’s heterogeneous etiologies and variable clinical trajectories, which often hinder timely risk stratification and targeted intervention for stroke patients. A growing body of research has delved into diverse categories of candidate biomarkers, encompassing inflammatory mediators, metabolic indicators, and blood cellular parameters and evaluated their potential in predicting short-term and long-term stroke outcomes such as functional independence, recurrence risk, and mortality. Through a narrative review of current literature, we have summarized key biomarkers such as C-reactive protein, interleukins, blood cells, lipid profiles, oxidative stress markers, microparticles and cell-free DNA, clarifying their associations with stroke pathophysiology and clinical endpoints. Simultaneously, we highlighted critical gaps and inconsistencies in existing studies, such as limited validation in multiethnic and underrepresented patient cohorts. Furthermore, we have discussed the practical clinical applications and inherent challenges of translating these biomarkers into real-world settings. Finally, we have proposed future research directions, emphasizing the development of standardized protocols, validation in large-scale prospective cohorts, and exploration of multiple biomarkers to address unmet clinical needs in stroke management. VL - 9 IS - 2 ER -
Department of Neurology, The First People’s Hospital of Jing Zhou and the First Affiliated Hospital of Yangtze University, Jing Zhou, China
Department of Neurology, The First People’s Hospital of Jing Zhou and the First Affiliated Hospital of Yangtze University, Jing Zhou, China;Department of Science and Education, The First People’s Hospital of Jing Zhou and the First Affiliated Hospital of Yangtze University, Jing Zhou, China
Department of Neurology, The First People’s Hospital of Jing Zhou and the First Affiliated Hospital of Yangtze University, Jing Zhou, China;Department of Stroke Center, The First People’s Hospital of Jing Zhou and the First Affiliated Hospital of Yangtze University, Jing Zhou, China
Department of Neurology, The First People’s Hospital of Jing Zhou and the First Affiliated Hospital of Yangtze University, Jing Zhou, China;Department of Stroke Center, The First People’s Hospital of Jing Zhou and the First Affiliated Hospital of Yangtze University, Jing Zhou, China
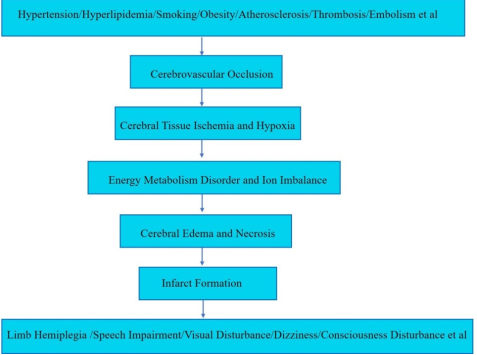
Figure 1.
Ischemic Stroke Pathogenesis and Clinical Manifestation.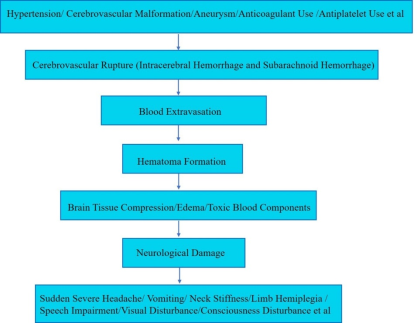
Figure 2.
Hemorrhagic Stroke Pathogenesis and Clinical Manifestation.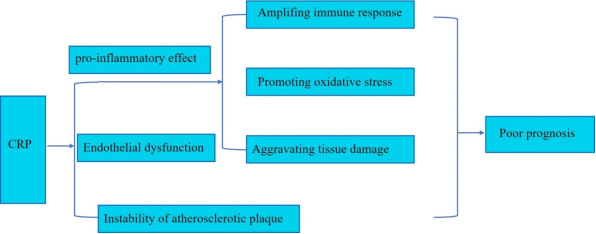
Figure 3.
Flowchart for CRP with prognosis.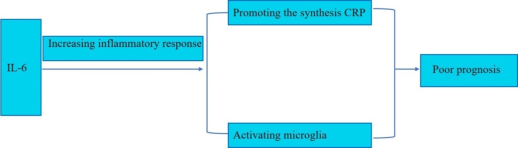
Figure 4.
Flowchart for IL-6 with prognosis.
Figure 5.
Flowchart for IL-10 with prognosis.
Figure 6.
Flowchart for NLR with prognosis.
Figure 7.
Flowchart for Lipid profiles with prognosis.
